
You are floating near the ceiling, looking down at your own body. The room is completely clear. You can see the medical team working, the angle of the overhead light, the specific position of the clock on the wall. You are not dreaming — the quality of clarity is wrong for dreaming. You are observing the scene with a calm you have never experienced before, from a perspective that is physically impossible, looking down at yourself from a height you cannot reach.
Approximately one person in ten will have an experience like this at least once. That is not a marginal figure. That is a documented, replicated finding across multiple large studies in multiple countries. Out-of-body experience — the sensation of consciousness located outside the physical body, observing it from an external position — is among the most common anomalous experiences reported by healthy people without any psychiatric diagnosis.
Neuroscience has identified the brain region most consistently implicated in producing it. It has also, in doing so, produced a finding more unsettling than the experience itself: the sense of being located inside your body is a construction. A fragile, actively maintained illusion generated by a specific cluster of neurons. When that cluster misfires, you leave.
"OBEs are related to a failure to integrate proprioceptive, tactile and visual information with respect to one's own body — and to a vestibular dysfunction leading to an additional disintegration between personal space and extrapersonal space."
— Olaf Blanke et al., "Out-of-body experience and autoscopy of neurological origin." Brain, 2004
The science is solid, detailed, and — at a certain point — runs out. The cases it cannot account for are the ones that have been documented most carefully.
The Territory
A Universal Experience With a Very Specific Address in the Brain
The out-of-body experience has been documented in ancient Egyptian texts describing the ba — the mobile soul that could leave the body during sleep or death and return to it. Tibetan Buddhist tradition developed an elaborate framework of consciousness projection in the bardo state. Shamanic traditions across Siberia, the Amazon basin, and West Africa built entire ritual practices around the deliberate induction of states in which the practitioner's consciousness left the body to travel and return with information. The consistent cross-cultural presence of OBE frameworks is not, itself, evidence that OBEs are anything other than a neurological event. It is evidence that they happen often enough, and reliably enough, to require cultural accommodation.
The psychical research tradition of the late 19th century documented OBEs extensively under the term "astral projection." Frederic Myers coined the term in this context. Robert Monroe brought the experience to a popular audience with his 1971 book Journeys Out of the Body — an account of his own recurring OBEs that became a foundational text for several decades of subsequent investigation. The Monroe Institute, founded on his research, continues to operate as a facility specifically devoted to OBE induction and study.
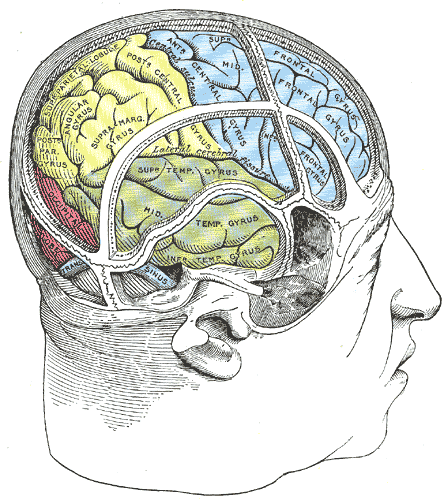
The neuroscientific breakthrough came in 2002, when Olaf Blanke and colleagues at EPFL published a paper in Nature describing the accidental induction of an OBE through direct electrical stimulation of a specific brain region in a 43-year-old epilepsy patient. They had been mapping the cortex before surgery. When they stimulated the right angular gyrus — a region at the junction of the temporal and parietal lobes, now known as the temporoparietal junction or TPJ — the patient immediately reported leaving her body and watching herself from above. When stimulation stopped, she returned. The experience was reproducible, on demand, by adjusting the current. The key to the self's location in the body had been found. Or so it appeared.
The Case Room
The Documented Encounters
The most important class of OBE for the purposes of this investigation is the near-death OBE — specifically, cases where the person reports accurate information about their physical environment that they could not have obtained through normal sensory channels while unconscious. These are the cases that the neurological model struggles with most directly.
Pam Reynolds was a 35-year-old musician who underwent surgery in 1991 for a giant brain aneurysm. The procedure — called hypothermic cardiac arrest — required her body temperature to be lowered to 60 degrees Fahrenheit, her heart stopped, her blood drained from her head, and her brain rendered electrically inactive as confirmed by EEG flatline. Her eyes were taped shut. Moulded ear inserts emitting continuous 100-decibel clicks were in place to monitor her brainstem — effectively blocking external sound. By any physiological measure, she was not conscious and could not perceive her environment. She later reported a detailed OBE during the procedure: she observed the saw used to open her skull, described it accurately as resembling a dentist's drill with detachable blades, heard a conversation about the size of her arteries, and observed the room from above the surgical team. Her description of the saw was later confirmed as accurate by the surgical staff. She had not seen surgical equipment before the operation and could not have described it from prior knowledge.
The Pam Reynolds case is perhaps the most studied single OBE on record. The neurologist Michael Sabom documented it in his 1998 book Light and Death, and it has been subjected to repeated sceptical analysis. The main counter-argument — that she could have gathered information about the surgical saw from prior exposure before she was sedated — has been examined carefully and not sustained. The saw is stored away from patient areas. Her description of its sound (comparing it to a musical tone) and visual appearance (dentist-drill-like with removable blades) matched the actual instrument with sufficient specificity that ordinary prior knowledge cannot account for it.
The broader NDE OBE literature contains numerous cases with a similar structure — verifiable observations made by an unconscious patient about the physical environment, later confirmed by staff. The AWARE study (AWAreness during REsuscitation), led by Dr Sam Parnia at the University of Southampton and subsequently at NYU, was designed specifically to test whether OBE claims during cardiac arrest could be verified by hidden targets — images placed face-up on high shelves, visible only from ceiling level — that resuscitated patients might report seeing during out-of-body episodes. The study ran for years across multiple hospitals. One verified case was recorded: a man reported floating near the ceiling during resuscitation, described the actions of staff accurately, and reported hearing a specific automated voice announcing shock delivery — which was later confirmed to have occurred at the time he was clinically dead by cardiac criteria.
One verified case in a multi-year study is not strong statistical evidence. It is not nothing, either. And the methodological challenge — that genuinely unconscious patients cannot report their experiences until they recover consciousness — means the AWARE study almost certainly under-recorded rather than over-recorded.
The connection to the other phenomena in this series is worth making explicit. The doppelganger involves the self appearing in a location the body is not. The bilocation cases involve the self confirmed present in two locations simultaneously. The OBE involves the self apparently leaving the body entirely and observing it from outside. These are different phenomenologies, but they share a structural assumption that current neuroscience cannot accommodate without discomfort: that consciousness and physical location are not, under all conditions, the same thing.
The Explanations
What Neuroscience, Consciousness Research and the Unresolved Record Say
The neurological model is the strongest available. The TPJ, when disrupted, produces the OBE — this is demonstrated, reproducible, and not in doubt. The model predicts the experience accurately: vestibular dysfunction produces the floating sensation; failure of multisensory body integration produces the observation of one's own body from outside; the supine position common in OBE accounts is consistent with the body posture during sleep or illness when the experience most commonly occurs. For the majority of OBEs — spontaneous, occurring during sleep or anaesthesia, without verifiable content — this explanation is adequate.
The problem is verifiable content. The Pam Reynolds case, the AWARE study case, and a body of NDE OBE reports from multiple independent researchers share a feature that the neurological model cannot currently explain: the person under anaesthesia or in cardiac arrest reports accurate observations about the physical environment that they could not have made through functioning sensory channels. If the experience is entirely generated by the disrupted brain, it should not contain accurate information about the external world. The fact that, in a subset of carefully documented cases, it does — is the gap that the neurological model has not closed.
Consciousness researchers including Thomas Metzinger have proposed that the OBE demonstrates something specific: that the self is a model, not a substance. The brain generates a model of being a self inside a body. When that model fails, the experience is of being outside it. This is philosophically significant — it suggests that the felt sense of inhabiting your body is an actively maintained construction rather than a direct perception — but it does not, by itself, explain verified external observations during states when the model-generating machinery should be offline.
Case Summary · Key Facts
- Approximately 10% of the general population report at least one OBE — a replicated finding across multiple international studies
- Blanke et al. (2002) demonstrated that direct electrical stimulation of the right temporoparietal junction (TPJ) reliably induces the OBE in awake patients
- Pam Reynolds case (1991): verifiable accurate observations during hypothermic cardiac arrest with confirmed EEG flatline — including description of a surgical instrument not previously seen
- AWARE study (Parnia et al.): one verified out-of-body observation during cardiac arrest confirmed across multi-year multi-hospital study
- OBE independently documented in Ancient Egyptian, Tibetan Buddhist, Siberian shamanic, West African, and Indigenous American traditions
- The neurological model explains the phenomenology of the experience; it does not account for verified external observations during unconscious states
- Status: Neurological mechanism identified. Verified-content cases remain unresolved.
The Open Door
What Leaves, and What Returns
This series has traced five phenomena that share a single unsettling implication: the self is not as fixed, as contained, or as singular as ordinary waking experience suggests. The doppelganger is seen outside the body. The Hat Man watches from the boundary between sleep and waking. The bilocating saint is confirmed present in two places. The vardoger precedes you through time. The OBE floats above the body and looks down.
Neuroscience has made genuine progress. The TPJ is real, its role in body ownership is documented, and the model of the self as a constructed representation rather than a substance is philosophically robust. What it has not done — and what the most carefully documented cases in this series make very hard to dismiss — is explain how a constructed representation that is offline can accurately observe the room.
One person in ten will leave their body at some point. Almost all of them will return. What they encountered in the interval between — and whether that interval is something more than a neurological misfire — is, for now, an open question. It is the same question this series has been asking from the beginning, wearing a different face.








